Internuclear ophthalmoplegia
When there is something in the frontal eye fields, a signal is sent to the paramedian pontine reticular formation, located in the pons. The signal is generated by Brodmann area 8, which houses the frontal eye fields, it's role is to initiate and guide eye movements towards objects of interest in the visual field. Broadmanns areas are distinct areas in the cortex. This sends a signal to cranial nerve VI, the abducens, nucleus, located in the pons. From this nucelus, there is both a contralateral and ipsilateral tract. The ipsilateral tract controls the lateral rectus on the respective side, and the contralateral connects to the contralateral nucleus of cranial nerve III in the midbrain. The tract runs through the medial longitudinal fasciculus. This is a white matter tract found in the pons and is typically affected by MS. Once CNIII is activated, an efferent fibre is sent to the medical rectus, which then allows for leftward and rightward gaze (lateral rectus will pull, while medial rectus will almost 'push').
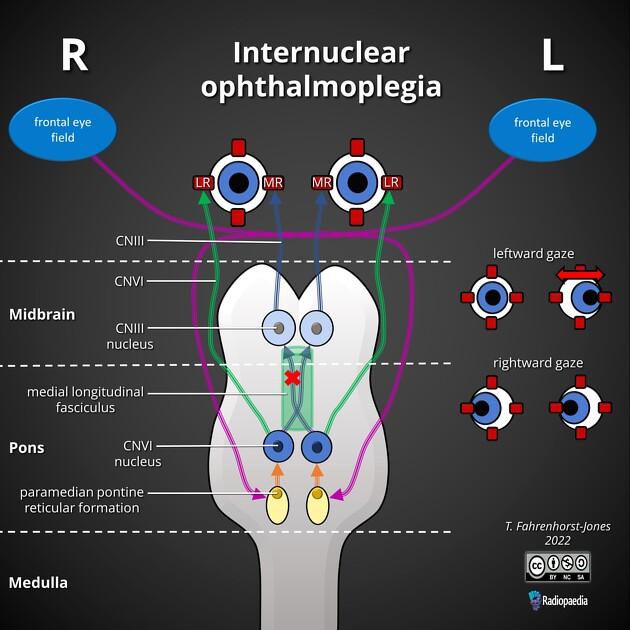
In intranuclear opthalmoplegia, the MLF is damaged, which means the contralateral pathway that supplies CNIII and eventually control of the medial rectus. When the pathway is damaged, the medial rectus can no longer perform its job, meaning there is no lateral gaze in the affected eye. A nystagmus is seen in the non-affected eye, which is a result of Hering's law of equal innervation; the 'weak' medical rectus prompts the cortex to increase innervation to it, resulting in excessive innervation to the contralaeral lateral rectus causing horizontal nystagmus.
INO plus syndromes
Result from more extensive lesions - there are multiple:
One and a half syndrome: Pontine lesion that involves the MLF and the CN VI nucleus or PPRF on the side of the eye with complete conjugate gaze palsy
Half-and-half syndrome: Involves MLF and also the CN VI fasciculus but spares the nucelus
Wall-eyed bilateral INO
Wall-eyed monocular INO
Paralytic pontine exotropia (PPE): Similar to one and a half syndrome
Non-paralytic pontine exotropia: Unclear but similar to one and a half syndrome with only a partia lesion of the ipsilateral PPRF
Seven-and-a-half syndrome: Lesion of the MLF and ipsilateral fasciular portion of the facial nerve
Eight-and-a-half syndrome
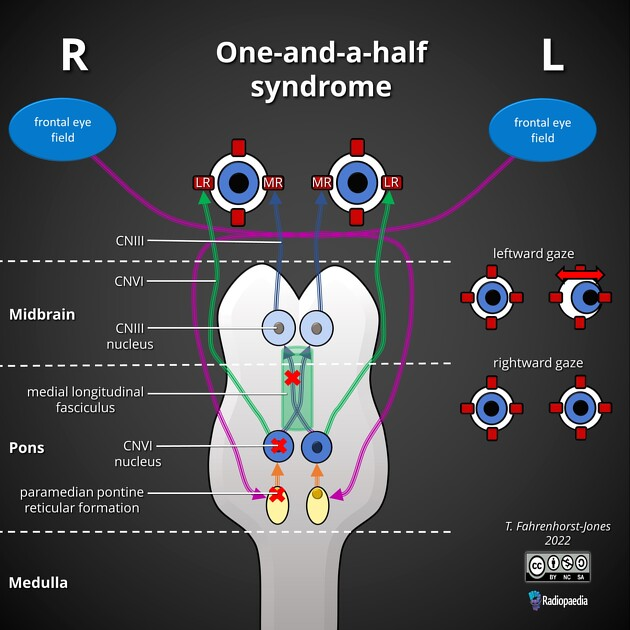
One and a half syndrome
In one and a half syndrome, the MLF is affected, which causes an classic INO. Alongside this, there is a lesion either in the nucelus of cranial nerve VI or the paramedian pontine reticular formation. They tend to be on the same side (if the right MLF is affected, the right CNVI nucelus/PPRF will be affected).
When the CN VI nucelus/PPRF is affected, there is no longer an ipsilateral tract from the CN VI nucelus to the lateral rectus, so the function is lost. This removes the ability for lateral gaze of the respective eye. As the CN VI/PPRF is affected, the contralateral pathway to CN III is also lost, thus affecting movement of the medical rectus on the contralateral side. If we then consider that the MLF is also affected, we lose the contralateral pathway from the other CNVI nucelus, removing the ability for the ipsilateral eye to move at all (the LR pathway is destoryed as the CN VI nucelus is destroyed, the MR pathway is destroyed due to the MLF lesion obstructing the pathway from the contralateral CNVI, so the ipsilateral CNIII is affected). This result in complete paralysis of lateral and medial gaze on the affected side, and a complete loss of medial gaze in unaffected side.